
This guide explains how the donor area is assessed, why graft numbers vary, what overharvesting means and why responsible treatment planning must consider future hair loss as well as the first procedure.
Introduction
People considering a hair transplant often begin by focusing on the area they want to restore. They may be concerned about a receding hairline, thinning through the mid-scalp, reduced density at the crown or an area of scar tissue.
The recipient area is important, but it is only one side of the procedure. The other is the donor area, where suitable follicles are removed before being transferred to the area affected by hair loss.
A hair transplant does not create new follicles. It redistributes the patient’s existing hair from one location to another. Every graft placed into the recipient area must therefore come from a limited donor supply.
This is why responsible planning should not begin with the largest possible graft number. It should begin with an assessment of the patient’s donor density, hair characteristics, scalp condition, medical history, pattern of loss and long term needs.
An overly aggressive procedure may improve the recipient area while leaving the donor region visibly thinner, uneven or scarred. It may also reduce the options available if natural hair loss continues.
Contents
- What is the donor area?
- Why donor hair is limited
- What a graft contains
- How the donor area is assessed
- Why graft numbers vary
- Hair characteristics and coverage
- Overharvesting and scarring
- Long term planning
- Beard and body hair
- Scar tissue and repair cases
- Graft survival and recipient planning
- Questions to ask during consultation
- Where IK Clinics fits
- Conclusion
What Is the Donor Area?
The donor area is the region from which hair follicles are taken for transplantation. For most scalp procedures, it is found around the back and sides of the head.
Hair within appropriate parts of this region may be more resistant to the biological processes involved in androgenetic hair loss. When suitable follicles are moved to a thinning area, they generally retain important characteristics associated with their original location.
However, not every hair at the back or sides of the scalp is permanently protected. The boundaries of the more stable donor region vary between individuals. Hair close to the upper, lower or forward edges may be more vulnerable to future thinning.
A clinical assessment must therefore consider more than whether hair is currently visible. The practitioner needs to examine whether the proposed donor region appears stable, whether miniaturisation is present and whether future hair loss may extend into the area being considered for extraction.
Donor and Recipient Areas
The recipient area is where the grafts are placed. It may include the hairline, temples, frontal scalp, mid-scalp, crown, beard, eyebrows or scar tissue.
Donor and recipient planning are closely connected. The size of the recipient area and the level of coverage being sought must be balanced against what the donor region can reasonably provide.
Where hair loss covers a large area, it may not be possible to create the same density throughout. The plan may need to prioritise certain regions, use a more conservative hairline or accept that complete coverage is not realistic.

Why Donor Hair Is Limited
A follicular unit removed from the donor area does not grow back in its original position.
The hairs surrounding the extraction site may continue growing, but the removed unit has been permanently relocated. The donor region therefore contains fewer follicles after surgery than it did before.
Follicular unit excision, usually known as FUE, distributes many small extraction sites across the donor area. These marks may be difficult to see when healing, hair length and surrounding density are favourable. However, FUE is not scarless.
Every extraction creates a permanent change. This does not make FUE inappropriate, but it does mean that the donor area must be used carefully.
Redistribution Rather Than Creation
Hair transplantation moves existing follicles rather than producing new ones.
A simple comparison is moving plants from a densely planted section of a garden into a sparse one. The sparse area may look fuller, but the original area will contain fewer plants. If too many are removed, the source area may begin to appear depleted.
Hair transplantation is more complex because follicular units contain different numbers of hairs and individual hair characteristics affect coverage. The central principle remains the same: the donor supply is finite.
Why a Large Donor Region Can Still Be Limited
A broad band of hair around the back of the head does not automatically mean that a large number of grafts can be removed safely.
Assessment may include follicular density, the number of hairs within each unit, hair calibre, scalp visibility, curl, colour contrast, miniaturisation, previous surgery, scarring and hairstyle preferences.
Hair that appears dense when grown longer may look much thinner when clipped closely. This is particularly relevant for patients who prefer short hairstyles.
What Does a Hair Graft Contain?
The words hair, follicle and graft are sometimes used interchangeably, but they do not mean exactly the same thing.
A follicular unit is a naturally occurring group of hairs. It may contain one, two, three or occasionally more hairs. A graft may contain one intact follicular unit, depending on the technique used.
This means two patients receiving the same graft number may receive a different total number of individual hairs.
One person may have a high proportion of multi-hair units, while another may have more single-hair units. Their final coverage may therefore differ even if the graft count is similar.
Single-hair grafts can be useful at the leading edge of the hairline because they create a softer appearance. Multi-hair units may provide more visual bulk behind the hairline or in areas where greater coverage is required.
Why Graft Numbers Do Not Predict the Result
Patients often ask how many grafts they need. This is understandable, but a number provided without examination can create false certainty.
The result depends on the size of the recipient area, the amount of existing hair, hair calibre, curl, contrast, the number of hairs within each graft, placement technique and future loss of natural hair.
Two patients receiving the same graft number may achieve very different levels of visible coverage.
Online graft calculators and estimates based only on photographs should therefore be treated cautiously. Photographs may support an initial discussion, but they cannot reliably show density, miniaturisation, scalp condition or donor stability.
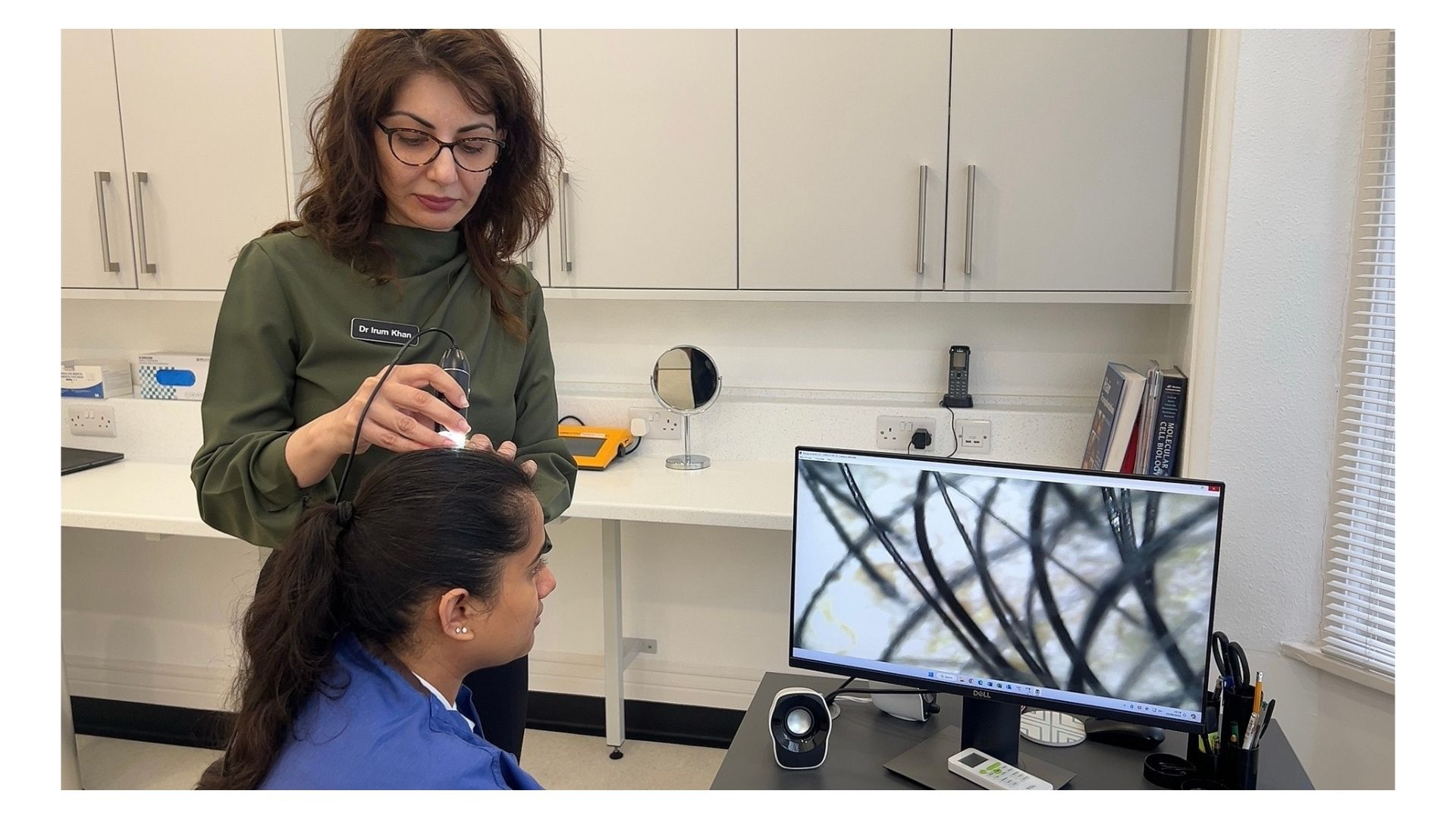
How Is the Donor Area Assessed?
Donor assessment should form part of a wider clinical evaluation.
The clinician may examine the scalp directly, assess density and hair characteristics, look for signs of scalp disease and review previous procedures. Medical history, medication, family history, symptoms and the rate of hair loss may also be relevant.
Donor Density
Donor density refers to the number of follicular units or individual hairs within a measured area.
A higher starting density may provide more flexibility, but it does not mean that unlimited extraction is safe. Even a dense donor region can become visibly thin if too many grafts are removed or if harvesting is concentrated within one area.
The pattern of extraction therefore matters as much as the total.
Miniaturisation and Stability
Miniaturisation occurs when affected follicles gradually produce finer and shorter hairs.
A donor area containing significant miniaturisation may be less stable than it first appears. Harvesting from such a region could transfer hairs that later become finer or are lost. The remaining donor hair may also continue to thin.
Miniaturisation requires professional interpretation and cannot be assessed reliably from a photograph alone.
Scalp Health
Inflammation, infection, active scarring conditions and other scalp problems may affect suitability, healing or the timing of surgery.
Hair loss does not always result from male or female pattern baldness. Some conditions need to be diagnosed and managed before cosmetic treatment is considered.
Persistent redness, scaling, pain, burning, itching or rapidly changing patches of hair loss should be discussed during assessment.
Previous Surgery
Previous FUE, FUT, scalp surgery or trauma can significantly alter the donor plan.
Earlier extraction may have reduced density unevenly, while a previous strip procedure may have left a linear scar. Repeated FUE sessions may also have caused widespread thinning.
The current condition of the donor area must therefore be assessed directly rather than relying only on historic graft numbers.
Hairstyle Preferences
Hair length can affect how visible extraction marks and reduced density become.
A donor area that looks well covered with longer hair may reveal more scalp when closely clipped. Patients should explain how they normally wear their hair and whether they intend to change their hairstyle after surgery.
Why Is There No Universal Safe Graft Number?
There is no single graft number that can be described as safe for every patient.
The appropriate extent of harvesting depends on donor density, follicular unit composition, hair calibre, curl, colour contrast, previous procedures, healing characteristics and future needs.
Published research provides frameworks for estimating donor capacity, but these should not be treated as universal consumer formulas.
A number that may be reasonable for one patient could leave another with visible thinning or scarring.
Distribution Matters
The total number of grafts removed is only part of the donor plan. Where and how those grafts are taken is equally important.
If extractions are concentrated too closely together, the remaining hair may no longer disguise the spaces and scars left behind. This can create a patchy or windowed appearance.
Responsible FUE harvesting aims to preserve visual uniformity. The goal is not simply to obtain grafts, but to protect the appearance and future usefulness of the donor area.
More Is Not Automatically Better
Large graft numbers can sound impressive in marketing, but a larger procedure is not necessarily a better one.
Responsible planning may involve treating a smaller area, choosing a more conservative hairline, staging treatment or advising against surgery where the donor supply is inadequate.
How Hair Characteristics Affect Coverage
The appearance created by transplanted hair depends on more than the number of grafts moved.
Hair calibre, curl, colour contrast and the number of hairs within each follicular unit all affect how easily the scalp can be seen.
Hair Calibre
Hair calibre refers to the thickness of each shaft.
Coarser hair usually creates more visual bulk than finer hair because each strand covers more space. Fine hair can still be transplanted, but expectations may need to be adjusted.
Removing more grafts simply to compensate for fine hair can place unnecessary pressure on the donor area.
Curl and Wave
Curly and wavy hair may create greater visual coverage because the shafts overlap and generate volume. Straight hair often lies flatter, making scalp visibility more noticeable.
Curl can also make extraction more technically demanding because the follicle beneath the skin may not follow the visible direction of the emerging hair.
Hair and Skin Contrast
The contrast between hair colour and scalp colour can affect how obvious spaces appear.
Dark hair against lighter skin may produce stronger contrast, making scalp visibility more noticeable. Where hair and skin tones are closer, the same density may appear fuller.
This is not a measure of suitability, but it can affect design and expectations.
What Is Donor Overharvesting?
Overharvesting occurs when follicular units are removed in a way that leaves the donor region visibly depleted, uneven or damaged.
It may result from taking too much from the total donor supply, concentrating extractions within a small area or extending into less stable regions.
The donor area may look generally thinner or develop patchy areas where more scalp becomes visible. Extraction marks may also become more noticeable, particularly with short hair.
Why Overharvesting Is Difficult to Correct
Overharvesting can reduce the number of follicles available for future treatment.
If natural hair loss continues or the original transplant requires refinement, there may no longer be enough suitable donor hair. The patient can then be left with both a depleted donor region and untreated hair loss elsewhere.
Repair may be possible in selected cases, but the options are often restricted by the shortage of remaining follicles.
Early Healing Changes
Redness, crusting, short hair and temporary shedding can make the donor area appear thinner during early healing.
These changes do not necessarily mean permanent overharvesting has occurred. Concerns should be assessed by the treating clinic at an appropriate stage of recovery.

Scarring and Healing
Every surgical hair transplant creates some form of scarring.
FUE produces multiple small extraction wounds, while FUT creates a linear scar where a strip of scalp has been removed.
Scar visibility depends on the technique, extent of surgery, healing response, hair characteristics and hairstyle. Describing FUE as entirely scarless can therefore create unrealistic expectations.
Healing can also be influenced by skin characteristics, smoking, medication, medical conditions, infection, trauma and adherence to aftercare. Patients should provide a full medical history and mention previous problems with scarring or wound healing.
Why Long Term Planning Matters
A hair transplant is performed at one point in time, but the result may be viewed for many years.
Transplanted follicles may retain much of the behaviour associated with their donor origin. The surrounding natural hair, however, may continue to thin.
A result that looks balanced today may appear isolated if recession develops behind it. A very low hairline may also use grafts that could later have been needed for the mid-scalp or crown.
Donor Budgeting
Donor budgeting means treating the available donor hair as a resource that may need to support the patient over the long term.
A plan may involve choosing a conservative hairline, prioritising the frontal scalp, accepting lower density in certain regions or delaying crown treatment.
This does not mean that every patient will require several procedures. It means possible future loss should be considered before a large proportion of the donor supply is used.
Age and Pattern of Loss
Younger patients may have patterns that are not yet fully established, making prediction more difficult. However, age alone does not determine suitability.
Family history, rate of progression, miniaturisation, diagnosis, treatment history and expectations must also be considered.
What Permanence Means
Hair transplants are often described as permanent because appropriately selected donor follicles tend to retain the resistance associated with their original location.
However, transplanted hair can still age or be affected by illness, medication, inflammation and other biological factors. Surgery also does not stop the future loss of untreated natural hair.
The long term appearance depends on both the transplanted follicles and what happens to the surrounding scalp.
Can Beard Hair Be Used as a Donor Source?
In selected patients, beard or body hair may be considered when the scalp donor supply is limited or a repair procedure requires additional options.
This does not make body hair a direct replacement for scalp hair.
Hair from different parts of the body may vary in calibre, curl, texture, colour, growth cycle and maximum length.
Beard-to-Scalp Transplantation
Beard hair is often coarser than scalp hair and may provide visual bulk in selected areas.
However, it may be less suitable for the soft leading edge of a hairline and may blend better when mixed with scalp hair further behind it.
The beard donor supply is also limited. Poorly planned removal can cause visible thinning, irregularity or scarring on the face or neck.
Other Body Hair
Chest and other body hairs may have a shorter growth phase and different maximum length from scalp hair.
Body hair transplantation has been used in selected advanced and repair cases, but the result may be less predictable. It should be treated as a specialist supplementary option rather than an unlimited reserve.
Scar Tissue and Repair Cases
Scar tissue may be present in either the donor or recipient area.
A patient may wish to soften a surgical, traumatic or burn scar with transplanted hair. Alternatively, the donor region may contain scars from previous FUE, FUT or another operation.
Transplanting Into Scar Tissue
Scar tissue may have altered blood supply, reduced flexibility and changes in thickness.
These factors can influence graft placement, healing and survival. Treatment may be possible in selected cases, but expectations may need to be more cautious.
Active inflammatory or scarring hair loss conditions require diagnosis and appropriate management before cosmetic transplantation is considered.
Repair Procedures
Repair procedures begin with whatever donor supply remains after previous surgery.
Some follicles may already have been removed, damaged or transplanted. The recipient area may also contain scarring or poorly positioned grafts.
This can make repair more complex and limit what can realistically be achieved. In some cases, modest improvement may be more appropriate than complete correction.

Graft Handling and Recipient Planning
Donor planning is not only about how many grafts can be removed. The grafts must also be protected, handled carefully and placed into suitable recipient tissue.
Survival may be affected by trauma during extraction, transection, dehydration, time outside the body, placement technique and the condition of the scalp.
Transection
Transection occurs when part of a follicle is unintentionally cut during extraction.
Excessive transection reduces the number of intact grafts available for implantation and may damage follicles left in the donor area.
Curl, scarring and variations in follicle direction can make extraction more technically challenging.
Recipient Density Has Limits
Placing more grafts into a small area does not automatically create better growth.
Grafts require tissue capable of supporting healing and revascularisation. Excessively dense placement, particularly in scarred or compromised tissue, may increase risk without producing the expected benefit.
The plan must balance cosmetic density with scalp condition, existing hair and the available donor supply.
Survival Claims
Precise or guaranteed graft survival percentages should be treated cautiously.
Outcomes vary, and lighting, styling, hair length and photography can affect the apparent result. A responsible consultation should explain the factors that influence growth without guaranteeing a particular outcome.
Planning Different Areas of the Scalp
The hairline, mid-scalp and crown have different planning requirements.
The Hairline
The hairline frames the face and strongly affects whether a result looks natural.
A very low hairline generally requires more grafts and may become difficult to support if recession continues. A mature and proportionate design can preserve donor supply and remain appropriate as the patient ages.
The Mid-Scalp
The mid-scalp connects the frontal region to the crown.
Using most of the donor supply at the front without considering the area behind it may create an uneven appearance if the central scalp continues to thin.
The Crown
The crown can cover a large area and contains a natural whorl pattern.
Restoring it at high density may require a substantial donor commitment. For some patients, prioritising the front and mid-scalp may create a greater cosmetic benefit than attempting full crown coverage.
Questions to Ask During Consultation
How Has My Donor Area Been Assessed? Ask whether density, miniaturisation, hair calibre, scalp health, previous surgery and future hair loss have been considered.
Is the Proposed Donor Area Stable? The clinician should explain why particular regions are being considered for extraction and whether future thinning could affect them.
How Will Extractions Be Distributed? It is reasonable to ask how concentrated harvesting and visible thinning will be avoided.
Why Has This Graft Number Been Suggested? The answer should relate to donor characteristics, the recipient area, hairline design and the long term plan.
How Might the Donor Area Look With Short Hair? Patients who prefer closely clipped hairstyles should discuss the possible visibility of extraction marks and reduced density.
What Happens if My Hair Loss Progresses? The plan should consider how the result may look if untreated natural hair continues to thin.
Could Beard or Body Hair Be Relevant? Alternative sources should only be discussed where appropriate. Patients should understand how the hair may blend and what effect extraction could have on the source area.
Who Performs Each Stage? Patients should know who is responsible for assessment, extraction, recipient site creation and graft placement.
What Are the Limitations and Alternatives? A balanced consultation should explain what surgery may not achieve, the relevant risks and whether non-surgical management or monitoring may be more appropriate.
Warning Signs in Donor Area Marketing
Patients should be cautious when marketing focuses more on graft volume than on suitability and donor preservation.
A graft number promised from photographs alone may not account for density, miniaturisation, scalp condition or stability. Recommending the same package to most patients may also suggest that individual differences are not being considered.
Claims that FUE is completely scarless, beard hair is unlimited or growth can be guaranteed should be treated carefully.
Where IK Clinics Fits
IK Clinics supports patients considering hair restoration through assessment, education and realistic planning.
For people considering hair transplant surgery in Leicester, the first step is not simply selecting a procedure or graft number. It is understanding whether surgery is appropriate and how the donor supply can be used responsibly.
A suitability discussion may consider the pattern and progression of hair loss, scalp condition, donor density, hair calibre, medical history, previous procedures, expectations, recovery, risks and long term planning.
Some patients may have a strong and stable donor area. Others may have fine hair, reduced density, miniaturisation, scar tissue, previous extraction or extensive recipient needs.
Beard hair may be relevant in selected cases, but it is not an automatic solution to limited scalp supply.
Assessment may also identify situations in which surgery should be delayed, modified or not recommended. Recognising these limitations is an important part of responsible care.
Conclusion
The donor area is the foundation of every hair transplant.
It contains a limited supply of follicles that must be balanced against the size of the recipient area, the patient’s hair characteristics and the possibility of future hair loss.
This is why graft planning should never be reduced to choosing the largest available number.
Density, calibre, curl, contrast, scalp health, scarring, hairstyle and previous procedures can all influence what may be appropriate. Beard and body hair may expand the options for selected patients, but these sources have their own limitations.
A responsible plan should improve the recipient area without unnecessarily depleting the donor region. It should also preserve reasonable options if the patient’s hair loss progresses.
An individual consultation is therefore essential before a personalised treatment plan can be recommended.

Related Reading
- Understanding Hair Graft Numbers: How Much Coverage Can You Expect?
- Exploring the Rise of Beard-to-Scalp Hair Transplants
- What Happens to Transplanted Hair After 10 Years?
- Hair Transplant Options for Different Hair Types
- Hair Transplants on Scar Tissue: Do They Work?
- Top Questions to Ask at Your First Hair Transplant Consultation
References
- NHS: Hair Transplant
A patient-friendly overview of hair transplant surgery, including the procedure, recovery, possible risks and what to consider when choosing a clinic. - British Association of Hair Restoration Surgery: Patient Advice
Guidance for patients researching hair transplant clinics, surgeons and treatment decisions. - British Association of Plastic, Reconstructive and Aesthetic Surgeons: Hair Transplant Surgery
An overview of hair transplant suitability, consultation, donor hair and surgical planning. - International Society of Hair Restoration Surgery: Is FUE Scarless?
Explains why FUE does not produce a linear scar but still creates small scars within the donor area. - Garg and Garg: Donor Harvesting Through Follicular Unit Excision
A clinical review of FUE donor harvesting, donor assessment, extraction and factors affecting graft quality. - Kerure and Patwardhan: Complications in Hair Transplantation
A peer-reviewed review covering possible donor and recipient area complications, including scarring, donor depletion and poor growth. - Saxena and Savant: Body-to-Scalp Hair Transplantation
A clinical review of the use of beard and other body hair as supplementary donor sources in selected patients. - International Society of Hair Restoration Surgery: Hair Restoration and the Scarred Scalp
Discusses the assessment of scar tissue, available donor hair and the factors affecting transplantation into scarred areas. - International Society of Hair Restoration Surgery: Body Hair Transplantation
An accessible overview of beard and body hair transplantation and the circumstances in which non-scalp donor hair may be considered. - Hair Transplant Practice Guidelines
Clinical guidance covering patient assessment, donor harvesting, treatment planning, surgical technique and patient safety.
Disclaimer
This article provides general educational information and is not a substitute for medical diagnosis, personalised treatment planning or advice from an appropriately qualified healthcare professional.
Hair loss can have many causes, and hair transplant surgery is not suitable for every person or every type of hair loss. Donor availability, surgical suitability, risks, expected coverage and likely long term outcomes can only be assessed through an individual consultation and clinical examination.
No specific graft number, treatment result or degree of permanence can be guaranteed. Seek professional medical advice if you are concerned about hair loss, scalp symptoms, an existing medical condition or the outcome of previous surgery.

