A receding hairline can feel like your face is quietly changing shape – and it’s no surprise it lands as one of the most common (and most stressful) hair concerns for both men and women.
So, can you stop it?
Not always. But in many cases, you can slow it down, stabilise it, and in some people, regain visible density – especially if you act early and treat the underlying cause rather than just the symptom.
Men vs women: same worry, different pattern
In men, a receding hairline is often part of male pattern hair loss (androgenetic alopecia) – the classic “corners going back” and/or thinning at the crown.
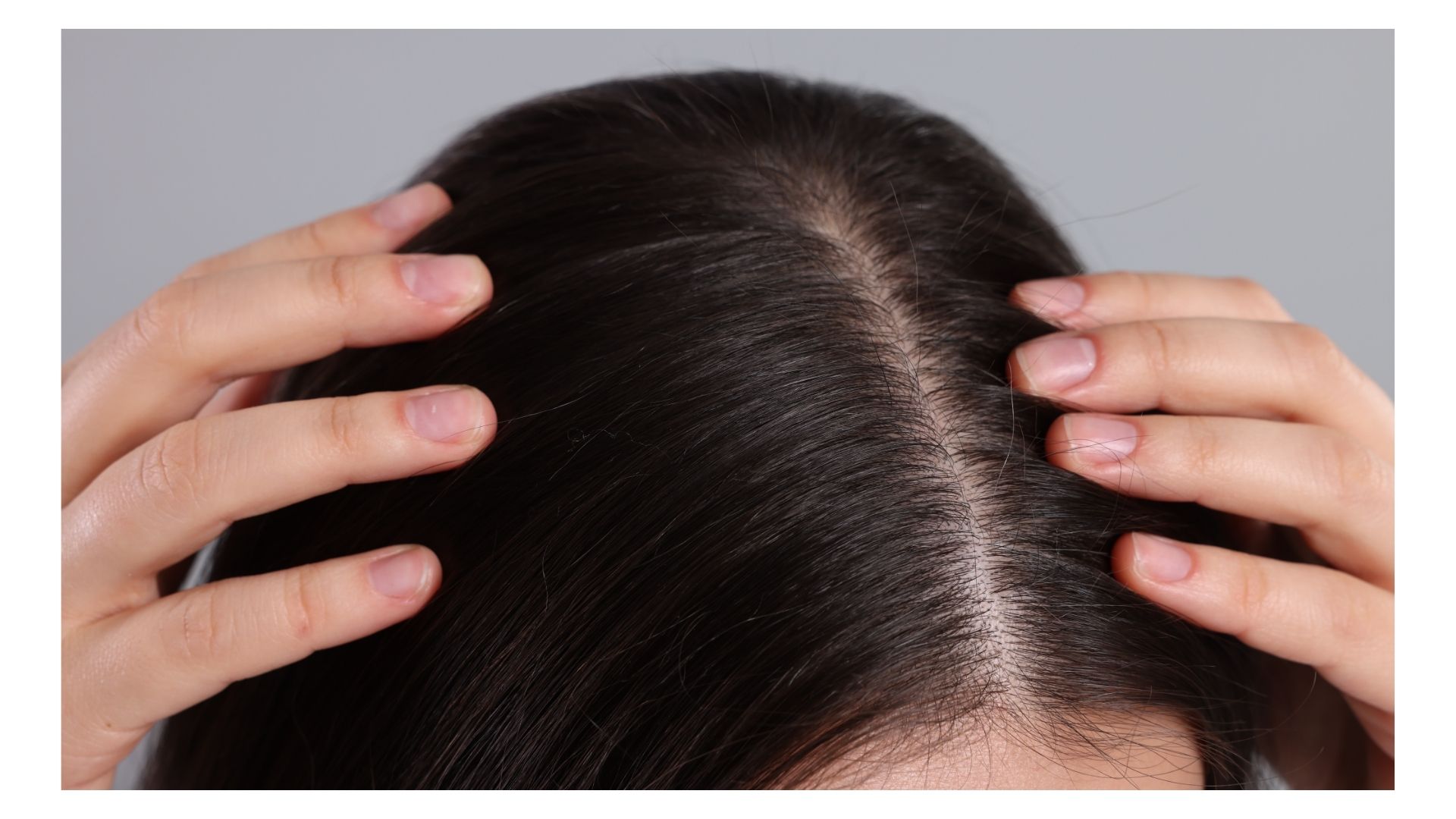
In women, it’s more common to see diffuse thinning over the top of the scalp, sometimes with the frontal hairline mostly preserved – though plenty of women do notice thinning at the temples or around the edges, depending on the trigger.
The biology behind typical pattern hair loss is a combination of genetics and hormones. One hormone, DHT (dihydrotestosterone), can drive a process called miniaturisation – follicles produce progressively finer, shorter hairs until growth slows dramatically.
But here’s the key point: not every “receding hairline” is genetic pattern hair loss. That’s why guessing (and panic-buying treatments) can waste months.
Step one is detective work: what’s actually causing your hairline to move?
A “hairline problem” can come from several different routes:
Pattern hair loss (genetics + hormones): gradual, progressive changes, often with family history.
Traction alopecia: repeated tension from tight hairstyles (tight ponytails, braids, extensions, weaves, head coverings under tension). Often worst at the front/temples, and may come with soreness or itching.
Stress-related shedding / telogen effluvium: more general shedding that can make the hairline look “emptier” even if follicles are still healthy.
Medical or nutritional factors (for example thyroid issues, iron deficiency, inflammatory scalp conditions) – which is one reason United Kingdom guidance suggests seeing a GP if you’re worried, ideally before jumping to commercial clinics.
In other words: stopping a receding hairline is sometimes about treatments – and sometimes about removing the thing that’s quietly pulling, shedding, or inflaming your hair in the first place.

Can you stop it? The honest answer
If genetics are doing the heavy lifting, you may not be able to “stop it” in the absolute sense – but you can often slow progression and protect what you still have, especially early on.
That’s a big win, because hair loss tends to be easier to treat when follicles are still producing hair (even if it’s thinner).
If the cause is traction, stress, or deficiencies, the outlook can be better – because removing the trigger can allow recovery (unless long-term traction has caused permanent follicle damage).
The “home front”: what you can do without a prescription
Lifestyle won’t outmuscle strong genetics on its own – but it can stop you accidentally accelerating hair loss.
Reduce tension and breakage. If your hairline is thinning around the edges, treat tight styles as a warning sign. The British Association of Dermatologists explicitly links traction alopecia to tight ponytails, buns, braids, extensions and similar styling, especially when combined with chemical treatments.
Support scalp health. Gentle cleansing, avoiding harsh treatments, and addressing flaking/inflammation can matter more than people think – inflammation can worsen shedding.
Stress management isn’t fluff. Many people notice increased shedding during prolonged stress. If you’ve had a big life event, illness, sleep disruption, or sustained anxiety, it’s worth considering that your hairline may be reflecting a broader “shedding season”.
Get the basics checked if it’s new, fast, or worrying. The NHS advises seeing a GP if you’re concerned about hair loss – especially because some causes are medical and treatable once identified.
Evidence-based treatments: what tends to work (and what the catch is)
Topical minoxidil (men and women). This is the best-known first-line option for many types of pattern hair loss. It can help in early stages, but it’s not a “one-and-done” fix: it requires consistent use, and benefits are generally maintained only while you keep using it.
The American Academy of Dermatology notes it can help early hair loss but won’t regrow an entire head of hair. One more detail people often misunderstand: a short-term increase in shedding can happen early on before things improve.
Finasteride (typically men; specialist-led in women). UK guidance lists finasteride among the main treatments for male pattern baldness, but it’s not suitable for everyone and only works while used.
It also comes with important safety considerations and potential side effects; authoritative prescribing information warns women who are pregnant or may become pregnant must not use it (and even handling broken tablets can be unsafe).
The NICE also flags mood-related adverse effects in prescribing guidance. Bottom line: this is a clinician conversation, not a casual add-to-basket.
Clinic options: PRP, lasers, and transplants – where they fit
PRP (platelet-rich plasma). PRP sits in the “promising, but variable” category. Meta-analyses have found improvements in hair density compared with placebo in androgenetic alopecia, but protocols vary (how it’s prepared, how often it’s done), which affects results.
If you’re considering it, ask clinics how they measure outcomes and what schedule they recommend.
Low-level laser/light therapy (LLLT). Systematic reviews of randomised trials suggest LLLT can improve hair outcomes in male and/or female pattern hair loss, and it’s often positioned as an add-on rather than a replacement for proven medications.
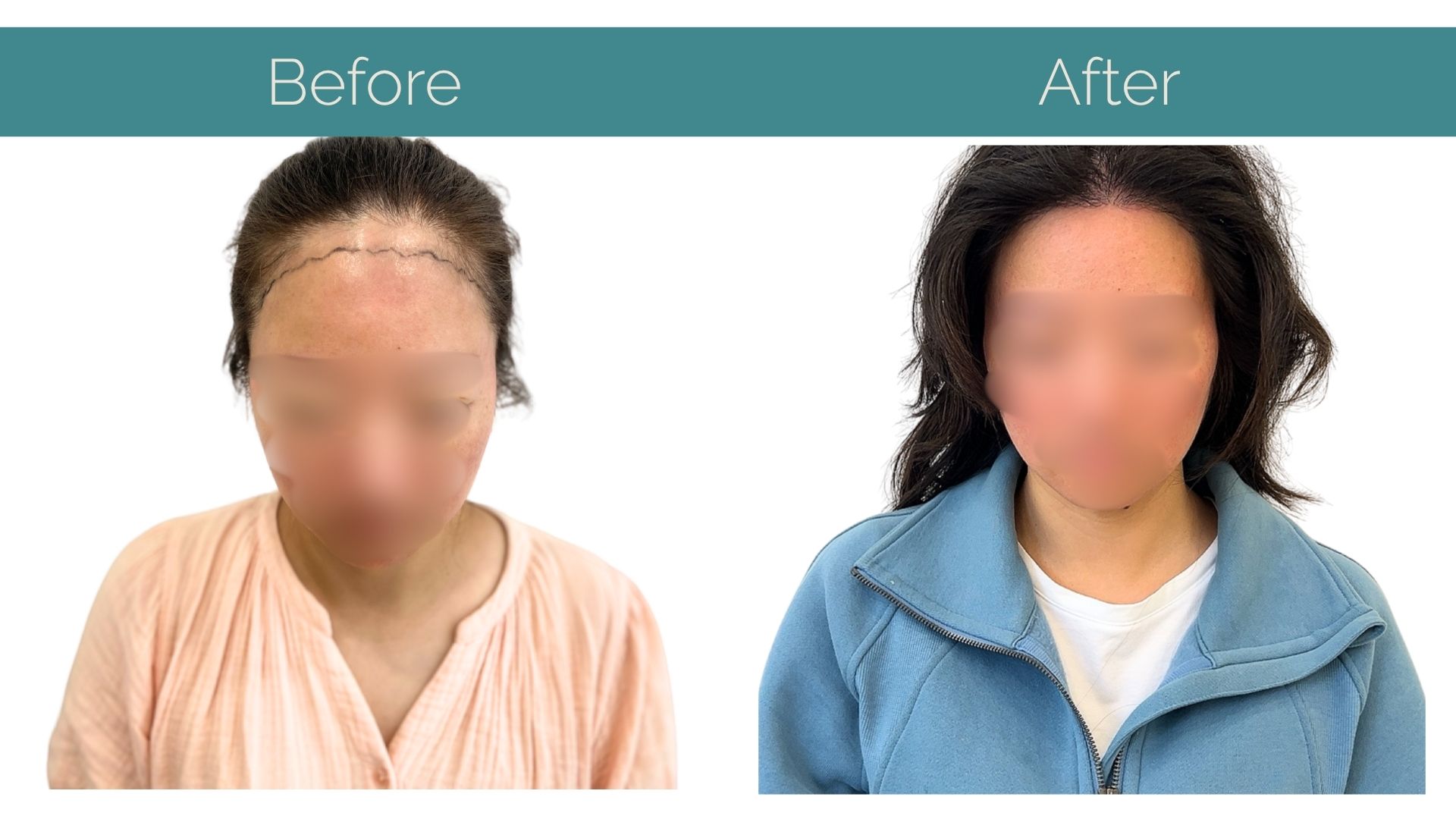
Hair transplant (when follicles are gone). If the hairline recession is advanced and you’re dealing with areas where follicles have essentially checked out, transplant surgery can be the most direct route to rebuilding a hairline.
It’s also the option that tends to feel “permanent” – though long-term planning matters, because surrounding native hair can continue thinning over time.
When to get help sooner rather than later
If hair loss is sudden, patchy, painful/itchy, or accompanied by other symptoms (fatigue, weight changes, menstrual/hormonal changes), don’t DIY it for months – get assessed.
And if your hairline is slowly changing but consistently, early intervention usually offers more options than waiting until it feels irreversible.
The takeaway
You might not be able to “stop” every receding hairline – but you can often slow it, stabilise it, and sometimes reclaim visible density, especially by (1) identifying the cause, (2) removing aggravators like traction and scalp stress, and (3) using treatments that match the diagnosis.
By taking control of your next steps and recognising the signs of hair loss, you can once again regain your confidence and get back on track to feeling like you again. With the right lifestyle changed, care plan and potential treatments, your youthful look can once again become a reality and not just a dream.

About IK Clinics
At IK Clinics, we are proud to stay at the forefront of global hair restoration trends, offering a variety of advanced techniques to meet the diverse needs of our clients. From FUE, PRP to Stem Cell Therapy, we ensure that every client’s treatment is tailored to their personal goals, helping them regain not just their hair but also their confidence.
Interestingly, we don’t just stop at hair restoration treatments, our highly skilled team also offers a range of anti-aging treatments.